THE DIFFERENT LAYERS
Nasal deformity requiring reconstruction results from a deficiency or (less commonly) an excess in at least one of the following 3 layers:
- Skin
- Framework
- Inner layer (lining)
In most cases, nasal deformity is the result of a deficiency caused by nasal cancer (skin or sinus cancer), severe trauma, or an inflammatory process that has changed the nose. To reconstruct the nose, we must make the correct diagnosis of what is too much or too little. Any of these excesses or deficiencies in each layer must then be addressed individually and returned to normal size and strength in order to properly reconstruct the nose. Unfortunately, there are no easier ways.
Using a comparison with a house as an imaginary symbol for the nose, we can say that the simplest layer to reconstruct is the ‘covering’ of the house. Covering the nose with borrowed skin from the forehead or cheek is generally not a complex procedure.
The next step is more complicated: reconstructing ‘the bricks of the house’ (the cartilage and bone). For this we take a small part of your rib or ear cartilage. This is trickier than ‘house re-cladding’ and requires careful sculpting of these fabrics. We only use your own tissue (autologous tissue), mainly from your rib or ear. Although we use cartilage from these areas, the shape of the ribs or ears remains the same.
The inner layer of the nose does not shape the nose and its function is to form a barrier against bacteria in your nose. Additionally, this layer provides blood flow to the framework, from the inner aspect of the nose. However, it is the most complicated layer to reconstruct. Using the ‘house comparison’, defects on the inside can be compared to defects in the foundations of a house. You will understand that faulty foundations in a house will lead to subsidence and instability of the entire structure on which it is built. It is therefore difficult and expensive to repair.
FACIAL & NASAL ASPECTS
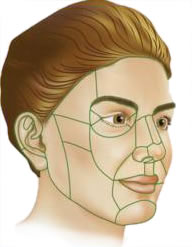
The shape of the nose varies from person to person. This is mainly due to the underlying middle bone and cartilage framework. The thickness of the skin also provides some contour. These aspects create a series of ‘gently rolling hills and valleys’. The transition from a convex to concave shape causes changes in light reflection and shadow formation, creating edges and transition zones. These areas have been defined by Burget and Menick as the aesthetic parts of the nose (Burget and Menick, 1985). The components of the nasal tip (hemi-), alar, dorsum and columella are convex, while the lateral walls of the nose and the soft triangle are concave.
In the edges/transition zones of the nose (as mentioned above), surgical incisions can be camouflaged for optimal cosmetic results. The distinction between concave and convex shapes is the key concept in the application of the ‘nose area principle’. In reconstructive situations involving 50% or more of a convex nasal area (tip, alar, columella and dorsum), a defect and its possible scarring can be concealed by incisions in the edges of the nasal areas.
This is the nasal areas principle (subunit principle) described by Burget and Menick in 1985.
ARE PERMANENT IMPLANTS USED IN OUR NOSE RECONSTRUCTIONS?
No. We absolutely do not use permanent synthetic implants such as polyethylene, polytetrafluoroethylene (PTFE) or Silastic in our nasal reconstructions. We believe that the use of these permanent implants in nasal reconstruction is not appropriate. Your reconstructed nose should not only last 5 or 10 years, as is the case with synthetic implants.
Using synthetic permanent implants may be an easier way to reconstruct a nose, but it exposes you to an ongoing risk of infection and extrusion (the implant coming through the skin) at a later date, sometimes as long as 15 to 20 years after surgery. If the extrusion of the implant occurs in a reconstructed nose, it can be a very difficult problem to correct.
Instead of a synthetic implant, we take the time to sculpt your own tissue (rib or ear cartilage) to replace the cartilage framework that is missing in your nose. In this way we try to minimize your risk of infection and reduce your risk of extrusion. We believe that the extra time and attention we invest in your nose reconstruction is very worthwhile.
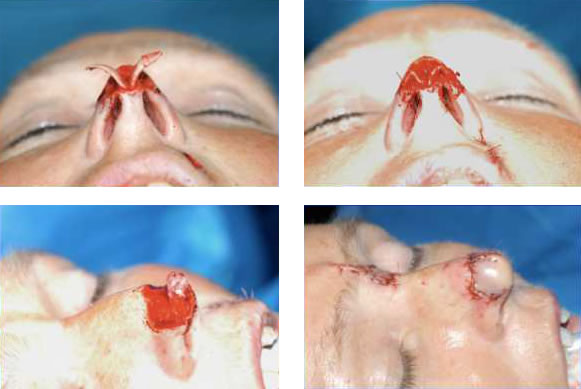
The photo shows a patient who has had the tip of his nose reconstructed using his own ear cartilage. The use of a permanent synthetic implant was therefore avoided. The skin of the forehead was used to cover the reconstructed nasal tip (nose).
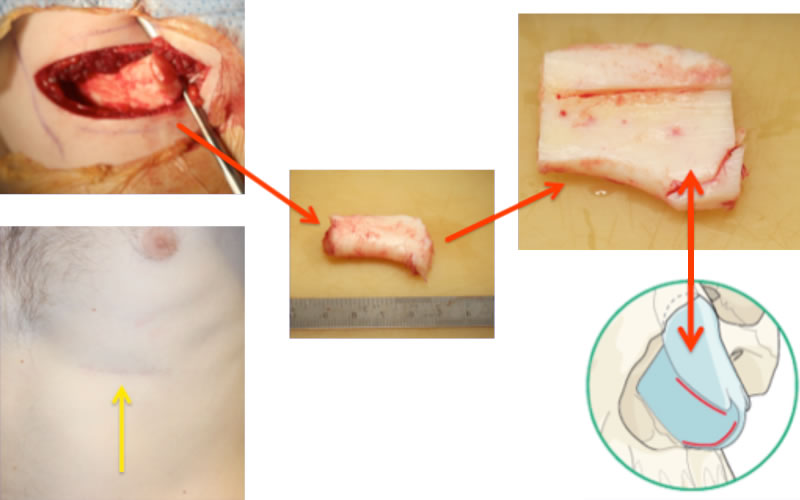
It is also possible to use costal cartilage and sculpt it appropriately to completely replace the septum and upper lateral cartilage of the nose (as indicated above with the red arrows). The yellow arrow indicates that the scar has healed. In women, this scar is hidden under the breast fold (without changing the shape of the breast).